Differences between groups were superimposed on a model MRI image.
Orange circles indicate areas of decreased gray matter density in the frontal and temporal lobes of patients with schizophrenia.
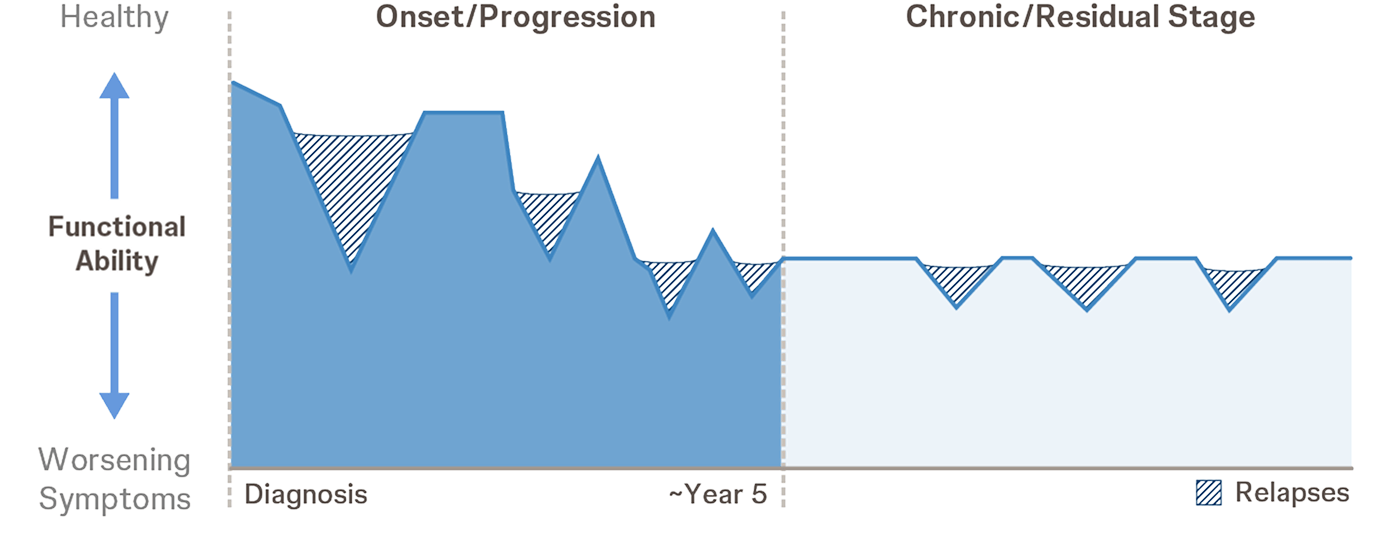
The first 3-5 years after a schizophrenia diagnosis are a critical period for patients. Disease progression during this period is often quite rapid, which can lead to worse patient outcomes.1
A comprehensive schizophrenia treatment plan will likely center on relapse prevention as a goal and measurement of success.2,3
20% homeless rate
in a study of patients with schizophrenia and other serious mental illnesses within a large public mental health system4
Suicides, drug overdoses, and accidents
account for most deaths in the younger schizophrenia population5
90% unemployment rate
in a population-based study of patients with schizophrenia and schizoaffective disorder6
Consistent Treatment Matters
Within 6 months posthospitalization,
7 out of 10
patients are nonadherent on oral antipsychotics7
According to a retrospective claims analysis of a multistate Medicaid database, adult patients taking LAls vs OAPs had:
65%lower riskof nonadherence7*†‡
In a Scandinavian longitudinal cohort analysis, use of an LAI vs an equivalent dose of an OAP was associated with:
33%lower riskof death8§
*Based on all LAIs and OAPs approved for use in the United States as of July 2013.
†Based on proportion of days covered <0.8.
‡Results presented here reflect a single claims analysis. other studies have not found a significant difference between LAIs and OAPs. Limitations: Some differences exist across groups despite attempts to minimize these; access issues may be a confounding variable, and adherence measures may overestimate OAP adherence. Other limitations included limited availability of data, lack of clinical severity measures or patient-reported self-measures, and data on duration of illness or prior treatment response.
§Based on all LAIs and OAPs approved for use in Sweden as of December 2013.
![]()
Actor portrayal.
Loss of Functional Ability Over Time10*
Differences between groups were superimposed on a model MRI image.
Orange circles indicate areas of decreased gray matter density in the frontal and temporal lobes of patients with schizophrenia.
More recent data are emerging that continue to explore the relationships between schizophrenia and cortical matter changes.14
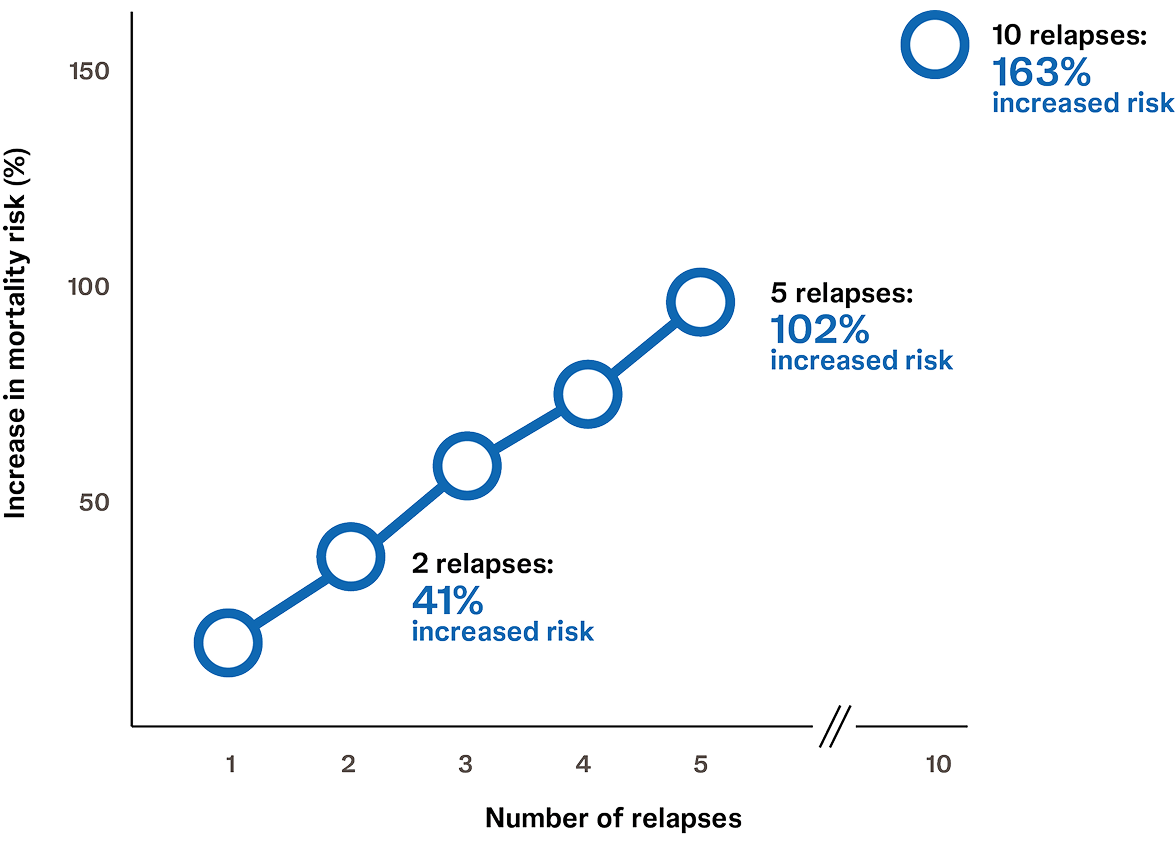
Recurring relapses in adult patients with schizophrenia are likely a cause of concern for members of their treatment team. In fact, a longitudinal database study of adults with stable schizophrenia found that risk of all-cause mortality increased with each schizophrenia relapse.22
![]()
Actor portrayal.
In the longitudinal study, each of the first 5 relapses increased all-cause mortality by approximately 20%22
LAI=long-acting injectable; OAP=oral antipsychotic.
*Adapted from Lieberman, et al. Am J Psychiatry. 2019
†Adapted from van Haren, et al. Neuropsychopharmacology. 2007.
References
1. Birchwood M. Early intervention and sustaining the management of vulnerability. Aust N Z J Psychiatry. 2000;34 Suppl:S181-S184. 2. Emsley R, Chiliza B, Asmal L, et al. The nature of relapse in schizophrenia. BMC Psych. 2013;13:50. 3. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia. Am J Psychiatry. 2020;177(9):868-872. 4. Folsom DP, Hawthorne W, Lindamer L, et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry. 2005;162(2):370-376. 5. Starzer MSK, Hansen HG, Hjorthøj C, et al. Predictors of mortality following a schizophrenia spectrum diagnosis: evidence from the 20-year follow-up of the OPUS randomized controlled trial. Schizophr Bull. 2023;49(5):1256-1268. 6. Evensen S, Wisløff T, Lystad JU, et al. Prevalence, employment rate, and cost of schizophrenia in a high-income welfare society: a population-based study using comprehensive health and welfare registers. Schizophr Bull. 2016;42(2):476-483. 7. Marcus SC, Zummo J, Pettit AR, et al. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J Manag Care Spec Pharm. 2015;21(9):754-768. 8. Taipale H, Mittendorfer-Rutz E, Alexanderson K, et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr Res. 2018;197:274-280. 9. Tandon R, Nasrallah H, Akbarian S, et al. The schizophrenia syndrome, circa 2024: what we know and how that informs its nature. Schizophr Res. 2024;264:1-28. 10. Lieberman JA, Small SA, Girgis RR. Early detection and preventive intervention in schizophrenia: from fantasy to reality. Am J Psychiatry. 2019;176(10):794-810. 11. Andreasen NC, Liu D, Ziebell S, et al. Relapse duration, treatment intensity, and brain tissue loss in schizophrenia: a prospective longitudinal MRI study. Am J Psychiatry. 2013;170(6):609-615. 12. Boonstra G, van Haren NE, Schnack HG, et al. Brain volume changes after withdrawal of atypical antipsychotics in patients with first-episode schizophrenia. J Clin Psychopharmacol. 2011;31(2):146-153. 13. van Haren NE, Hulshoff Pol HE, Schnack HG, et al. Focal gray matter changes in schizophrenia across the course of the illness: a 5-year follow-up study. Neuropsychopharmacology. 2007;32(10):2057-2066. 14. Howes OD, Cummings C, Chapman GE, et al. Neuroimaging in schizophrenia: an overview of findings and their implications for synaptic changes. Neuropsychopharmacology. 2023;48(1):151-167. 15. Zhao Y, Zhang Q, Shah C, et al. Cortical thickness abnormalities at different stages of the illness course in schizophrenia: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(6):560-570. 16. Chand GB, Dwyer DB, Erus G, et al. Two distinct neuroanatomical subtypes of schizophrenia revealed using machine learning. Brain. 2020;143(3):1027-1038. 17. Remington G, Foussias G, Agid O, et al. The neurobiology of relapse in schizophrenia. Schizophr Res. 2014;152(2-3):381-390. 18. van Erp TG, Hibar DP, Rasmussen JM, et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol Psychiatry. 2016;21(4):547-553. 19. Roiz-Santiañez R, Suarez-Pinilla P, Crespo-Facorro B. Brain structural effects of antipsychotic treatment in schizophrenia: a systematic review. Curr Neuropharmacol. 2015;13(4):422-434. 20. Nasrallah HA. Triple advantages of injectable long acting second generation antipsychotics: relapse prevention, neuroprotection, and lower mortality. Schizophr Res. 2018;197:69-70. 21. Radua J, Borgwardt S, Crescini A, et al. Multimodal meta-analysis of structural and functional brain changes in first episode psychosis and the effects of antipsychotic medication. Neurosci Biobehav Rev. 2012;36(10):2325-2333. 22. Correll CU, Bookhart BK, Benson C, et al. Association of relapse with all-cause mortality in adult patients with stable schizophrenia. Int J Neuropsychopharmacol. 2025;28(5):pyaf018.